Chronic Granulomatous Disease (CGD) Symptoms and Sequelae
CGD Specialty Center
Review the radiographic images below to better understand how infections and granulomas may present in patients with CGD.
Osteomyelitis, hepatic abscess, and lymphadenitis may be signs of chronic granulomatous disease.1
Autoimmune disorders are common in CGD. Some autoimmune diseases reported in individuals with CGD include juvenile idiopathic arthritis, autoimmune pulmonary disease, and myasthenia gravis.1
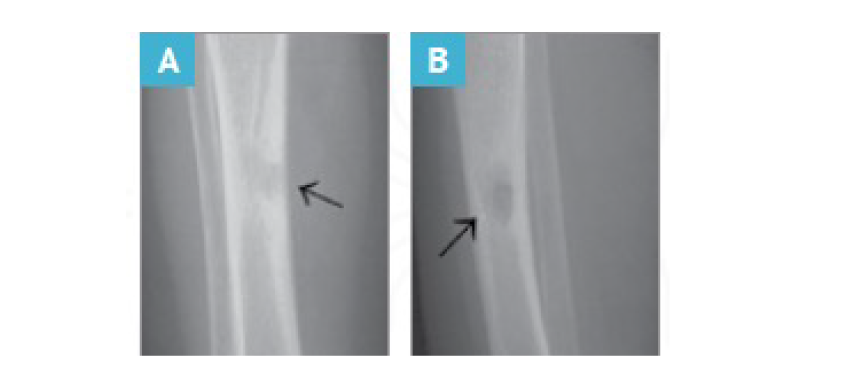
Osteomyelitis in a patient aged 4 years with CGD who presented with a limp.3
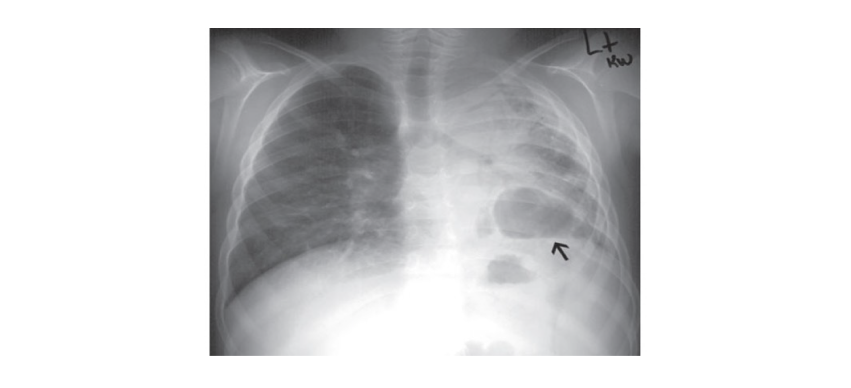

8-year-old patient with CGD presenting with pulmonary infection, fever, and respiratory distress.3
Infections and granulomatous lesions are usually the first manifestations of CGD, with the skin being among the most frequently impacted sites.1
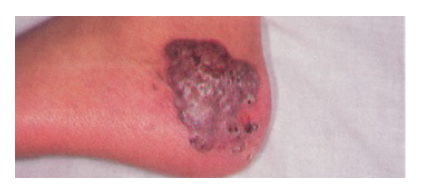

Granulomatous plaque of cutaneous aspergillosis located on the left foot in a patient aged 13 years with CGD.2
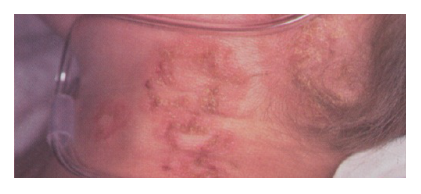
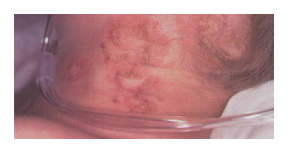
Vesicular lesions present in an 8-year-old boy with X-linked CGD. The vesicles measured 2 mm to 3 mm and were located predominantly on the neck and torso.2
Gastrointestinal symptoms indicative of CGD may include pyloric edema, abdominal pain, diarrhea, and perirectal granulomas.1
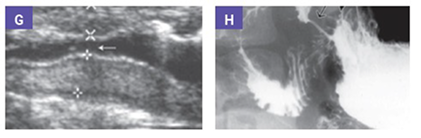
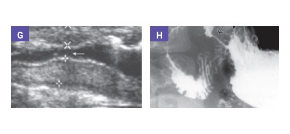
Gastric outlet obstruction in a symptomatic boy aged 9 years with CGD.3
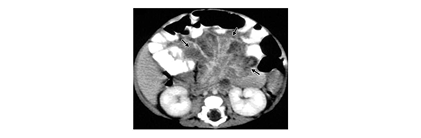

2-month-old CGD patient presenting with intra-abdominal infection, fever, and protuberant abdomen.3
The most frequent sites of infection, common infectious complications, and location of common inflammatory complications due to CGD include1:


Early diagnosis is beneficial for patients with CGD because they are susceptible to serious infections.1,4* If CGD is suspected, a dihydrorhodamine (DHR) test can confirm a diagnosis.

Look for pathogens that may indicate CGD
Many severe infections in patients with CGD in North America are caused by a select group of organisms, both bacterial and fungal.1,5-10 Most of these pathogens, including Aspergillus, Nocardia, Serratia, Burkholderia, Klebsiella, and Staphylococcus aureus, are catalase-positive.5,6 In patients with CGD, these catalase-positive pathogens are noteworthy because they can neutralize some of the hydrogen peroxide produced by neutrophils other than those in nicotinamide adenine dinucleotide phosphate (NADPH) oxidase.6
Most frequent pathogens and common presentations associated with CGD†

Aspergillus species are the most common cause of invasive fungal infections.1
Common presentation: pneumonia, lymphadenitis, osteomyelitis, brain abscess
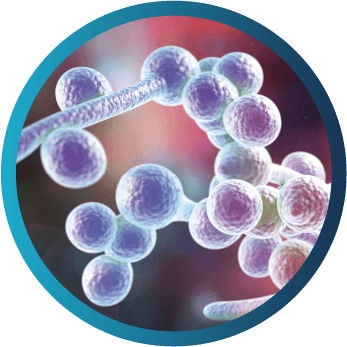
Candida species‡
Common presentation: sepsis, soft tissue infection, liver abscess
Staphylococcus aureus, Burkholderia cepacia complex, Serratia marcescens, and Nocardia species are the primary causes of most infections in individuals with CGD.1,9

Nocardia species
Common presentation: pneumonia, osteomyelitis, brain abscess

Serratia marcescens
Common presentation: osteomyelitis, soft tissue infections; less common presentation: pneumonia, sepsis

Burkholderia (formerly pseudomonas) cepacia complex
Common presentation: pneumonia, sepsis

Klebsiella species
Common presentation: pneumonia, skin infections, lymphadenitis
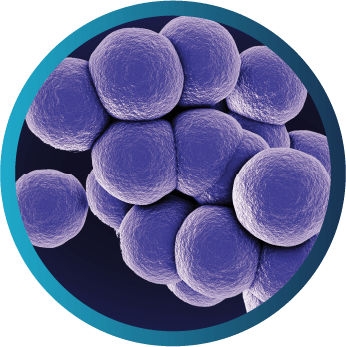
Staphylococcus aureus
Common presentation: soft tissue infections, lymphadenitis, liver abscess, perirectal abscess, osteomyelitis, pneumonia, sepsis
-
*Serious infection is defined as a clinical event requiring hospitalization and/or intravenous antibiotics.
†This is not a complete list of pathogens. Infections may also be caused by other species of bacteria and fungi not listed here.
‡Candida is most commonly reported in the EU.
Speak with a representative to learn more about CGD sequelae
Learn how to interpret DHR histograms when testing for CGD
-
References:
1. Leiding JW, Holland SM. Chronic granulomatous disease. In: Pagon RA, Adam MP, Ardinger HH, et al, eds. GeneReviews®. Washington, Seattle: University of Washington, Seattle; 1993-2022. 2. Dohil M, Prendiville JS, Crawford RI, Speert DP. Cutaneous manifestations of chronic granulomatous disease. A report of four cases and review of the literature. J Am Acad Dermatol. 1997;36(6 pt 1):899-907. 3. Khanna G, Kao SC, Kirby P, Sato Y. Imaging of chronic granulomatous disease in children. Radiographics. 2005;25(5):1183-1195. 4. Holland SM. Chronic granulomatous disease. Clin Rev Allergy Immunol. 2010;38(1):3-10. 5. Bonilla FA, Khan DA, Ballas ZK, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. J Allergy Clin Immunol. 2015;136(5):1186-1205.e1-e78. 6. Bortoletto P, Lyman K, Camacho A, et al. Chronic granulomatous disease: a large, single-center US experience. Pediatr Infect Dis J. 2015;34(10):1110-1114. 7. Leiding JW, Malech HL, Holland SM. Clinical Focus on Primary Immunodeficiencies: Chronic Granulomatous Disease. Immune Deficiency Foundation; 2013. 8. Marciano BE, Zerbe CS, Falcone EL, et al. X-linked carriers of chronic granulomatous disease: Illness, lyonization, and stability. J Allergy Clin Immunol. 2018;141(1):365-371. 9. Song E, Jaishankar GB, Saleh H, Jithpratuck W, Sahni R, Krishnaswamy G. Chronic granulomatous disease: a review of the infectious and inflammatory complications. Clin Mol Allergy. 2011;9(1):10-24. 10. van den Berg JM, van Koppen E, Ahlin A, et al. Chronic granulomatous disease: the European experience. PLoS One. 2009;4(4):e5234.